Board of Licensure for Professional Engineers and Land Surveyors Complaint Form
INSTRUCTIONS: ALABAMA BOARD OF LICENSURE FOR PROFESSIONAL ENGINEERS AND LAND SURVEYORS COMPLAINT FORM
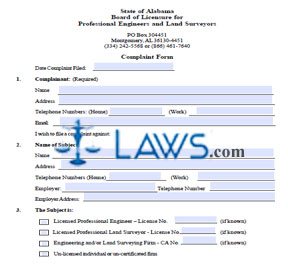
To file a complaint against an Alabama professional engineer, land surveyor, or engineering or land surveying firm, use the document discussed in this article. This form may be obtained from the website of the Alabama Board of Licensure for Professional Engineers and Land Surveyors.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 1: Enter the date on which the complaint is being filed.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 2: In section 1, provide your name, address, home and work telephone numbers and email address.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 3: In section 2, provide the name, address, home and work telephone numbers, email address, employer name, address and telephone number of the subject you are filing a complaint against.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 4: In section 3, indicate whether the subject is a engineer, land surveyor or firm with a check mark.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 5: In section 4, indicate what your complaint concerns with a check mark.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 6: In section 5, provide all details requested about your complaint.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 7: In section 6, provide a brief description of your complaint. If necessary, attach additional numbered and signed sheets.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 8: In section 7, list supportive documents such as copies of court orders, receipts and canceled checks.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 9: In section 8, list the name, address and telephone number of all other known parties with direct interest in this case or who can provide pertinent information.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 10: In section 9, state what you want done to remedy this situation.
Alabama Board Of Licensure For Professional Engineers And Land Surveyors Complaint Form Step 11: In section 10, indicate whether you have entered or anticipate litigation regarding this matter with a check mark.