
Form UCR-1 Unified Carrier Registration 2011
INSTRUCTIONS: CONNECTICUT UNIFIED CARRIER REGISTRATION – YEAR 2011 (Form UCR-1)
To register multiple motor vehicles used as carriers in a unified way, use a form UCR-1. This document can be obtained from the website of the government of Connecticut.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 1: Section 1 concerns general information. In the first five blank boxes, enter your US Department of Transportation number, your MC number, your FF number, your telephone number and your fax number.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 2: In the next two blank boxes, enter your business legal name and email address.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 3: In the next blank box, enter your "doing business as" (dba) name.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 4: In the next blank box, enter the street address of your principal place of business.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 5: In the next three blank boxes, enter your principal business city, your principal business state and the zip code.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 7: In the next blank box, enter your mailing street address.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 8: In the next three blank boxes, enter your mailing city, state and address.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 9: In section 2, indicate with a check mark whether you are a motor carrier, a motor private carrier, a broker, a leasing company or a freight forwarder.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 10: Section 3 concerns fees due for brokers, freight forwarders and leasing companies only. If this applies to you, you should also skip to Section 7 at this time.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 11: Section 4 is for motor carriers and private motor carriers only. Document the number of motor vehicles as directed.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 12: Section 5 concerns the few owed based on the number of vehicles.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 13: Enter the total fees due in Section 6.
Connecticut Unified Carrier Registration – Year 2011 UCR-1 Step 14: Print and sign your name in section 7, as well as entering your title and the date.
Form P-142N Neurology Medical Report
INSTRUCTIONS: CONNECTICUT NEUROLOGY MEDICAL REPORT (Form P-142N)
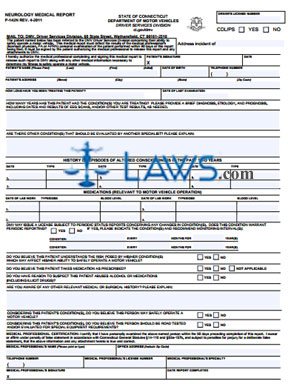
When a Connecticut driver has been involved in an incident that may be related to a neurological condition, they may be required to be examined by a medical professional. This examination is documented using a form P-142N. This document can be obtained from the website of the government of Connecticut.
Connecticut Neurology Medical Report P-142N Step 1: Write the date of the incident being addressed.
Connecticut Neurology Medical Report P-142N Step 2: The patient should sign and date the first two blank boxes, then submit the form to the medical professional evaluating them for completion.
Connecticut Neurology Medical Report P-142N Step 3: Enter the patient's name, date of birth and telephone number in the first three blank boxes.
Connecticut Neurology Medical Report P-142N Step 4: Enter the patient's street address, city, state and zip code in the next blank box.
Connecticut Neurology Medical Report P-142N Step 5: In the next two blank boxes, enter how long you have been treating this patient and the date of their last examination.
Connecticut Neurology Medical Report P-142N Step 6: In the next blank section, enter how many years the patient has had this condition, as well as providing a brief diagnosis, etiology and prognosis.
Connecticut Neurology Medical Report P-142N Step 7: In the next blank section, write whether the patient has any other conditions which should be evaluated by another specialist. If so, provide an explanation.
Connecticut Neurology Medical Report P-142N Step 8: In the table provided below, document episodes of altered consciousness in the last two years. Enter the date and type of each episode.
Connecticut Neurology Medical Report P-142N Step 9: In the table provided below this, document medications relevant to motor vehicle operation as instructed.
Connecticut Neurology Medical Report P-142N Step 10: Indicate whether the condition warrants periodic reporting with a check mark. If so, write the condition and the frequency with which periodic status reports should be issued in months, as well as the duration of years for which these reports should continue.
Connecticut Neurology Medical Report P-142N Step 11: Answer all remaining questions by checking "yes" or "no" as applicable.
Connecticut Neurology Medical Report P-142N Step 12: Print and sign your name at the bottom of the page, as well as providing all other identifying information requested.
Form – Bd Eval Professional Engineer Licensure Request for Board Evaluation of Transcript Related Science

INSTRUCTIONS: ALABAMA PROFESSIONAL ENGINEER LICENSURE REQUEST FOR BOARD EVALUATION OF TRANSCRIPT RELATED SCIENCE (Form Bd Eval/ENG)
Alabama graduates of four year science programs related to engineering who completed their studies before December 31, 2005 may use the form discussed in this article to request a professional engineer license. This document can be obtained from the website maintained by the Alabama Engineers and Land Surveyors Board.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 1: On the first six blank lines, enter the universities you attended and the degrees received.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 2: On the next blank line, print your name.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 3: On the next two blank lines, enter your address.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 4: On the next blank line, enter the date.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 5: On the next blank line, enter your daytime phone number, including the area code.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 6: On the next blank line, indicate whether you have filed a Fundamentals of Engineering (FE) or Professional Engineer (PE) with this board before.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 7: The rest of the form requires documentation of relevant classes taken. For each category of class, enter the title of the course in the first column, the course number in the second column, the hours in the third column, your grade in the fourth column, and the university where your degree was completed in the fifth column. The first section is for documentation of required math courses.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 8: The second section is for documentation of optional math classes.
Alabama Professional Engineer Licensure Request For Board Evaluation Of Transcript Related Science Bd Eval/ENG Step 9: On the last page, document your basic sciences classes.