Health Insurance and Optional Enrollment Application
INSTRUCTIONS: ALABAMA HEALTH INSURANCE AND OPTIONAL ENROLLMENT APPLICATION
Alabama public education employees who wish to enroll in the state's health insurance plan known as PEEHIP do so using the form discussed in this article. This document can be obtained from the website of the Retirement Systems of Alabama.
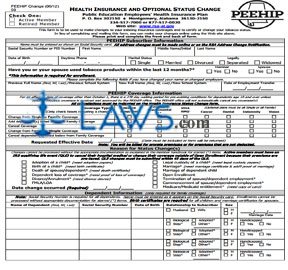
Alabama Health Insurance And Optional Enrollment Application Step 1: Indicate with a check mark whether you are an active member or retired.
Alabama Health Insurance And Optional Enrollment Application Step 2: The first section concerns subscriber information. Enter your Social Security number, full name, mailing address, date of birth, home and work phone numbers, gender, marital status, the name of your employer and school system, your email address and date of employment.
Alabama Health Insurance And Optional Enrollment Application Step 3: Indicate with a check mark whether you or your spouse have made use of tobacco products within the last 12 months.
Alabama Health Insurance And Optional Enrollment Application Step 4: The next section concerns the type of coverage you are seeking. Indicate with a check mark whether you are applying for hospital/medical coverage, supplemental hospital/medical coverage, or a VIVA health plan. If the latter, indicate with a check mark whether you are seeking it as a single person or for a family.
Alabama Health Insurance And Optional Enrollment Application Step 5: Indicate with check marks all additional optional coverages you are seeking and enter your requested effective date.
Alabama Health Insurance And Optional Enrollment Application Step 6: The next section requires anyone seeking family coverage to document their dependents. Enter each dependent's name, Social Security number and date of birth. Indicate their gender and relationship to you with check marks.
Alabama Health Insurance And Optional Enrollment Application Step 7: The next section is to be completed if seeking PEEHIP Supplemental coverage or if you or your dependents currently have other group health, dental or vision coverage in effect.
Alabama Health Insurance And Optional Enrollment Application Step 8: The next section must be completed if you or your dependents are eligible for Medicare.
Alabama Health Insurance And Optional Enrollment Application Step 9: The next section is only for completion by PEEHIP members who retired after September 30, 2005.
Alabama Health Insurance And Optional Enrollment Application Step 10: Sign and date the bottom of the form.