Hospital Medical Claim Form - Group 61000 and 14000
INSTRUCTIONS: HOSPITAL MEDICAL CLAIM FORM - GROUP #61000 AND #14000
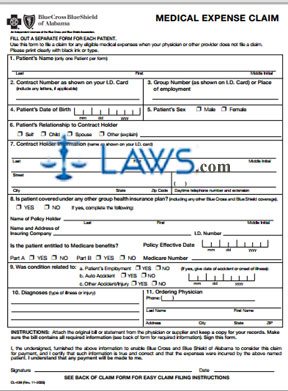
Alabama public employees enrolled in BlueCross/BlueShield groups 61000 and 14000 use the claim form discussed in this article to seek payment for services provided by a physician or pharmacy. This document can be obtained from the website maintained by the Retirement Systems of Alabama.
Hospital Medical Claim Form - Group #61000 And #14000 Step 1: In box 1, enter the patient's last name, first name and middle initial.
Hospital Medical Claim Form - Group #61000 And #14000 Step 2: In box 2, enter the patient's contract number as shown on their identification card. If there are any letters in this contract number, include them.
Hospital Medical Claim Form - Group #61000 And #14000 Step 3: In box 3, enter the patient's group number as shown on their card or their place of employment.
Hospital Medical Claim Form - Group #61000 And #14000 Step 4: In box 4, enter the patient's date of birth.
Hospital Medical Claim Form - Group #61000 And #14000 Step 5: In box 5, indicate the patient's sex with a check mark.
Hospital Medical Claim Form - Group #61000 And #14000 Step 6: In box 6, indicate with a check mark the patient's relationship to the contract holder.
Hospital Medical Claim Form - Group #61000 And #14000 Step 7: In box 7, give the contract holder's name as shown on their identification card, street address, city, state, zip code and daytime telephone number, including any applicable extension.
Hospital Medical Claim Form - Group #61000 And #14000 Step 8: If the patient is covered under any other group health insurance form or is entitled to Medicare benefits, box 8 should be completed. Otherwise, leave this box blank.
Hospital Medical Claim Form - Group #61000 And #14000 Step 9: In box 9, indicate with check marks whether the condition being treated was related to the patient's employment, an auto accident or another type of accident or injury. If yes, give the date on which the accident occurred or illness began.
Hospital Medical Claim Form - Group #61000 And #14000 Step 10: In box 10, give the patient's diagnoses.
Hospital Medical Claim Form - Group #61000 And #14000 Step 11: In box 11, give the ordering physician's phone number, name and address. Sign and date the form.